Odontogenic tumors are lesions derived from the epithelial and/or mescnchymal remnants of the toothforming apparatus. They are therefore found exclusively in the mandible and maxilla (and occasionally gingiva) and must be considered in differential diaenoses of lesions involving these sites. The etiology and pathogenesis of this group of lesions are unknown. Clinically, odontogenic tumors are typically asymptomatic, although they may cause jaw expansion, movement of teeth, root resorption, and bone loss. Knowledge of typical basic features such as age, location, and radiographic appearance of the various odontogenic tumors can be extremely valuable in developing a clinical differential diagnosis. Like neoplasms elsewhere in the body, odontogenic tumors tend to mimic microscopically the cell or tissue of origin. Histologically, they may resemble soft tissues.
EPITHELIAL TUMORS
Ameloblastoma
Pathogenesis
This neoplasm originates within the mandible or maxilla from epithelium that is involved in the formation of teeth. Potential epithelial sources include the enamel organ, odontogenic rests (rests of Malassez, rests of Serres), reduced enamel epithelium, and the epithelial lining of odontogenic cysts, especially dentigerous cysts. The trigger or stimulus for neoplastic transformation of these epithelial residues is totally unknown. Mechanisms by which ameloblastomas gain a. growth and invasion advantage include overexpression of antiapoptotic proteins (Bcl-2, Bcl-xL) and interface proteins (fibroblast growth factor [FGF], matrix metalloproteinases [MMPs]). Ameloblastomas, however, have a low proliferation rate, as shown by staining for the cell cycle-related protein, Ki-67. Mutations of the p53 gene do not appear to play a role in the development or growth of ameloblastoma.
Clinical Features
Ameloblastoma is chiefly a lesion of adults. It occurs predominantly in the fourth and fifth decades of life, and the age range is very broad, extending from childhood to late adulthood (mean age, approximately 40 years). The rare lesions occurring in children are usually cystic and appear clinically as odontogenic cysts. There appears to be no gender predilection for this tumor. Ameloblastomas may occur anywhere in the mandible or maxilla, although the mandibular molarramus area is the most favored site. In the maxilla the molar area is more commonly affected than the premolar and anterior regions. Lesions are usually asymptomatic and are discovered either during routine radiographic examination or because of asymptomatic jaw expansion. Occasionally, tooth movement or malocclusion may be the initial presenting sign.
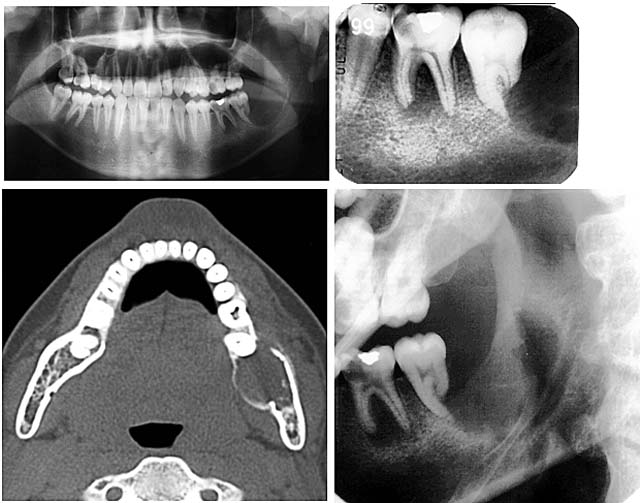
Radiographically, ameloblastomas are osteolytic, typically found in the tooth-bearing areas of the jaws, and may be either unilocular or multilocular. Because ameloblastomas are slow growing, the radiographic margins are usually well defined and sclerotic. In cases in which connective tissue desmoplasia occurs in conjunction with tumor proliferation, ill-defined radiographic. margins are typically seen. This variety, known as desmoplasticameloblastoma, also has a predilection for the anterior jaws and radiographically resembles a fibroosseous lesion. The generally slow tumor growth rate may also be responsible for the movement of tooth roots. Root resorption occasionally occurs in association with ameloblastoma growth.

 ameloblastoma of mandible producing marked cortical expansion
ameloblastoma of mandible producing marked cortical expansion


Biologic Subtypes
Peripheral or extraosseous amelobtastomas may occur in the gingiva and very rarely in the buccal mucosa. These lesions are seen in older adults, usually between 40 and 60 years of age. They may arise from overlying epithelium or rests of Serres. They exhibit a benign, nonaggressive course and generally do not invade underlying bone. Following local excision, recurrence is rare.
Malignant variants of ameloblastomas may rarely be encountered. These lesions occur in a relatively young age-group (thirties) and appear in the mandible more commonly than in the maxilla. By definition, these are lesions that metastasize to local lymph nodes or distant organs. Direct extension into contiguous areas does not qualify' for a malignant classification. Malignant lesions have been divided into two subtypes: malignant ameloblastoma , in which the primary and metastatic lesions are microscopically well differentiated with the characteristic histologic features of ameloblastoma, and ameloblastic carcinoma, in which the lesions (primary and/or metastatic) exhibit less microscopic differentiation, showing cytologic atypia and mitotic figures. Malignant variants of ameloblastomas are difficult to control locally. Metastases may appear usually in the lung, presumably because of aspiration of tumor cells. Regional lymph nodes are the second most common metastatic site, followed by the skull, liver, spleen, kidney, and skin.
An epithelial odontogenic malignancy of the mandible and maxilla that is believed to arise from odontogenic rests has been designated as primary intraosseous carcinoma. This lesion does not have histologic features of ameloblastoma and is regarded as a primary jaw carcinoma. It docs not have its origin from a preexisting odontogenic cyst. This rare lesion of adults affects men more than women, and it is seen in the mandible more than the maxilla. Microscopically, about half of these lesions exhibit keratin formation and about half show peripheral palisading of epithelial cell nests. This lesion must be differentiated microscopically from acanfhomatous ameloblastoma and squamous odontogenic tumor. The prognosis is poor, with a 2-year survival rate reported at 40%.
Another ameloblastoma that might be considered a subtype has been designated as sinonasal ameloblastoma. A mean age of 61 years and male dominance have been noted. Signs of nasal obstruction, epistaxis, and opacification are seen. The "totipotential" sinonasal lining cells are the putative cells of origin. A plexiform microscopic pattern is most commonly seen.
Histopathology
Numerous histologic patterns of no clinical relevance may be seen in solid ameloblastomas. Some may exhibit a single histologic subtype; others may display several histologic patterns within the same lesion. Common to all subtypes is the palisading of columnar cells around epithelial nests in a pattern similar to that of ameloblasts of the enamel organ. Central to these cells are loosely arranged cells that mimic the stellate reticulum of the enamel organ. Another typical feature is the budding of tumor cells from neoplastic foci in a pattern reminiscent of tooth development.
The microscopic subtype most commonly seen in solid ameloblastoma is the follicular type. It is composed of islands of tumor cells that mimic the normal dental follicle. Central cystic degeneration of the follicular islands leads to a microcystic pattern. The neoplastic cells occasionally develop into a network of epithelium, prompting the term plexiform ameloblasloma. When the stroma is desmoplastic and the tumor islands become squamoid or elongated, the term desmoplastic ameloblastoma is used. Some tumors are microscopically similar to basal cell carcinoma and are called basal cell or basaloid ameloblastomas. A type of solid ameloblastoma in which the central neoplastic cells exhibit prominent cytoplasmic granularity (and swelling) is known as granular cell ameloblastnma. Clear tumor cells and cells expressing ghost cell-type keratinization have also been seen in ameloblastomas. Separation of ameloblastomas into the various microscopic groups described is essentially within the same lesion. Common to all subtypes is the palisading of columnar cells around epithelial nests in a pattern similar to that of ameloblasts of the enamel organ. Central to these cells are loosely arranged cells that mimic the stellate reticulum of the enamel organ. Another typical feature is the budding of tumor cells from neoplastic foci in a pattern reminiscent of tooth development. The microscopic subtype most commonly seen in solid ameloblastoma is the follicular type. an academic exercise, because there appears to be no correlation between clinical behavior and these microscopic patterns.
Cystic ameloblastoma is a type of ameloblastoma. that has a major cystic space or spaces lined by thin epithelium showing basal palisading. There is often epithelial imagination into supporting connective tissue, and occasionally, mural islands may be seen. There is also a characteristic spongiotic change in the epithelial lining, and occasionally subepithelial hyalini/ ation. Some lesions have an intraluminal component, usually in a plexiform pattern. Diagnosis is often retrospective after enucleation for what was thought to be an odontogenic cyst.
 (A) Keratocystic odontogenic tumor showing moderate reactivity in prickle cells (B) Follicular ameloblastoma showing strong reactivity in peripheral columnar cells (C) Plexiform ameloblastoma showing strong reactivity in peripheral columnar cells (D) Ameloblastic carcinoma showing strong reactivity in tumor cells (× 400).
(A) Keratocystic odontogenic tumor showing moderate reactivity in prickle cells (B) Follicular ameloblastoma showing strong reactivity in peripheral columnar cells (C) Plexiform ameloblastoma showing strong reactivity in peripheral columnar cells (D) Ameloblastic carcinoma showing strong reactivity in tumor cells (× 400).
 follicular ameloblastoma
follicular ameloblastoma
Cystic ameloblastoma is a type of ameloblastoma. that has a major cystic space or spaces lined by thin epithelium showing basal palisading. There is often epithelial imagination into supporting connective tissue, and occasionally, mural islands may be seen. There is also a characteristic spongiotic change in the epithelial lining, and occasionally subepithelial hyalini/ ation. Some lesions have an intraluminal component, usually in a plexiform pattern. Diagnosis is often retrospective after enucleation for what was thought to be an odontogenic cyst.




Differential Diagnosis
When age, location, and radiographic features are considered together, the clinical differential diagnosis can generally be limited to several entities in the three categories of jaw disease— odontogenic tumors, cysts, and benign nonodontogenic lesions. Among the odontogenic tumors the radiolucent form of the calcifying epithelial odontogenic tumor and odontogenic myxomas are prime considerations. The dentigerous cyst and the odontogenic keratocyst can also be included. In relatively young individuals, lesions that are radiographically similar to ameloblastoma include nonodontogenic lesions such as central giant cell granuloma, ossifying fibroma, central hemangioma, and possibly idiopathic histiocytosis.
Treatment and Prognosis
No single standard type of therapy can be advocated for patients with ameloblastoma. Rather, each case should be judged on its own merits. Of prime considerations are whether the lesion is solid, cystic, extraosseous, or malignant, and location. The solid lesions require at least surgical excision, because recurrence follows curettage in 50% to 90% of cases. Block excision or resection is generally reserved for larger lesions. Cystic ameloblastomas may be treated less aggressively, but with the knowledge that recurrences are often associated with simple curettage. Peripheral ameloblastomas should be treated in a conservative fashion. Malignant lesions should be managed as carcinomas. Patients with all forms of central ameloblastoma should be followed indefinitely, since recurrences may be seen as long as 10 to 20 years after primary therapy. Ameloblastomas of the maxilla are generally more difficult to manage than those of the mandible due to anatomic relationships and due to the high content of cancellous bone in the maxilla. Thus intraosseous maxillary ameloblastomas are often excised with a wider normal margin than mandibular tumors.
Radiotherapy has rarely been used in the treatment of ameloblastomas, because it is generally believed that these tumors are radioresistant. Until more is known about tumor responsiveness, radiation should be reserved for exceptional cases that are difficult or impossible to control surgically.
Surgery help for reasons innumerable.From cosmetic value to hard medical reasons surgery is taken to for cure and relief.Thanks for posting about the surgical relieves.
ReplyDeletesinus surgery Los Angeles
Good post..thanx fr the valuable in formation..y don't you read the case report on CEOT?and gather more knowledge..here : http://dentistryandmedicine.blogspot.com/2010/12/calcifying-epithelial-odontogenic.html
ReplyDeleteGood post..thanx fr the valuable in formation..y don't you read the case report on CEOT?and gather more knowledge..here : http://dentistryandmedicine.blogspot.com/2010/12/calcifying-epithelial-odontogenic.html
ReplyDeleteI am very much delighted. To everyone reading this,i want to inform the public on how i got cured from stage 2 ovarian cancer by Dr Itua Herbal Medicines. i have been suffering from ovarian cancer, and i have also taken treatment from my doctor but no way out,few weeks back i came on the internet to see if i will be able to get any information as to curing Cancers, on my search i saw various testimony of people who was healed from Uterine Cancers and Brain Tumors by the good doctor, called Dr Itua. without any hesitation, i contacted his email: drituaherbalcenter@gmail.com and i wrote him and and he guided me,i asked him for solutions and he started the remedies for me so i started using the medicine, after the period of three weeks given to me by Dr Itua i was completely cured nomore tumors on my body was found anymore. So dear viewer why living your life in therapist or chemo?contact him now on WhatsApp +2348149277967 he is able to cure the listed diseases:Arthritis,Amyotrophic Lateral Scoliosis,Brain Tumor,Fibromyalgia,Pancreative Cancer,Fluoroquinolone ToxicityBladder cancer,Brain cancer,Hiv,Herpes,Esophageal cancer,Kidney cancer,Gallbladder cancer,Gestational trophoblastic disease,Head and neck cancer,Hodgkin lymphoma,Thyroid Cancer,Uterine cancer,Fibroid,Angiopathy, Ataxia,
ReplyDeleteIntestinal cancer,Hpv,Lung cancer,Melanoma,Mesothelioma,Multiple myeloma,Neuroendocrine tumors
Non-Hodgkin lymphoma,Oral cancer,Ovarian cancer,Sinus cancer,Hepatitis,Skin cancer,Soft tissue sarcoma,Spinal cancer,Stomach cancer,Leukemia,Liver cancer,Vaginal cancer,Vulvar cancer,Alzheimer's disease,Chronic Diarrhea,Copd,Parkinson,Als,Adrenocortical carcinoma Infectious mononucleosis.
Testicular cancer,Tach Diseases,Throat cancer,Ocd,
Syndrome Fibrodysplasia Ossificans ProgresSclerosis,