Mucocele is a clinical term that includes mucus extravasation phenomenon and mucus retention cyst. Because each has a distinctive pathogenesis and microscopy, they are considered separately. Ranula is a clinical term that also includes mucus extravasation phenomenon and mucus retention cyst, but it occurs specifically in the floor of the mouth. Ranula is associated with the sublingual or submandibular glands and presents as a fluctuant, unilateral,soft tissue mass. It often exhibits a bluish color that has been compared to a frog's belly; hence the term ranula. When it is significantly large, it can produce medial and superior deviation of the tongue. It may also cross the midline if the retained mucin dissects through the submucosa. A deep, so-called plunging ranula develops if mucus herniates through the mylohyoid muscle and along the fascial planes of the neck. On rare occasions it may progress into the mediastinum.
The Salivary glands Disease which are included into Reactive Lesions:
1. Mucus Extravasation phenomenon/ Mucocele
2. Mucus Retention cyst/ Ranula
3. Maxillary Sinus Retention Cyst/ Pseudocyst
4. Necrotizing Sialometaplasia
5. Adenomatoid Hyperplasia
1. Mucus Extravasation Phenomenon
Etiology and PathogenesisThe cause of mucocele is traumatic severance of a salivary gland excretory duct, resulting in mucus escape, or extravasation, into the surrounding connective tissue. An inflammatory reaction of neutrophils followed by macrophages ensues. Granulation tissue forms a wall around the mucin pool, and the contributing salivary gland undergoes inflammatory change. Ultimately, scarring occurs in and around the
gland.
gland.
Clinical Features
The lower lip is the most common site of mucocele, but the buccal mucosa, anterior-ventral surface of the tongue (location of Blandin-Nuhn glands), floor of the mouth, and retromolar region are often affected. Lesions are uncommonly found in other intraoral regions where salivary glands are located, probably because of a lower susceptibility to trauma. Mucus extravasation phenomenon presents as a relatively painless smooth-surfaced mass ranging in size from a few millimeters to 2 cm in diameter. It has a bluish color when mucin is superficially located. Adolescents and children are more commonly affected than adults. Lesions may fluctuate in size because of mucosal rupture over the pooled mucin. Continued production of mucin leads to recurrence. The maximum size is usually reached within several days after injury, and a viscous material is found if aspiration is attempted. Superficial mucocele is a variant of the extravasation type mucocele. Rather than arising from traumatic duct rupture, this form of mucocele is believed to arise as a result of increased pressure in the outer most part of the excretory duct. These lesions are asymptomatic and numerous, occurring most commonly in the retromolar area, soft palate, and posterior buccal mucosa. Their clinical appearance suggest a vesiculobullous disease, but the lesions persist for an extended time. Other than being a diagnostic challenge, they are of little significance.

Histopathology
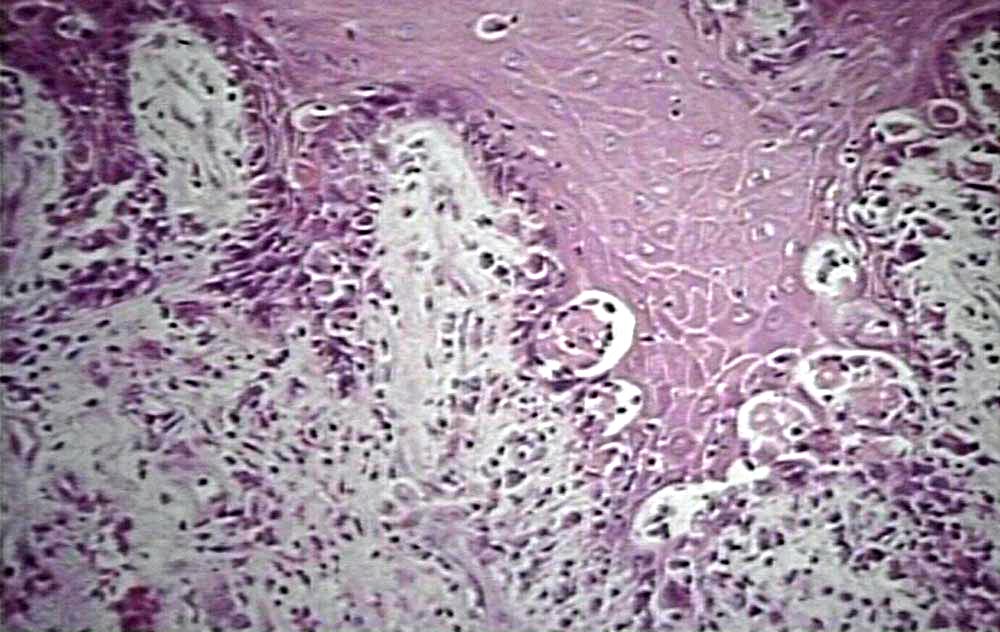
Extravasation of free mucin incites an inflammatory response that is followed by connective tissue repair. Neutrophils and macrophages are seer and granulation tissue forms around the mucin pool. The adjacent salivary gland whose duct was transected shows ductal dilation, chronic inflammation, acinar degeneration, and interstitial fibrosis.

histopathologic image of extravasation type mucocele from lower lip

Differential Diagnosis
Although a history of a traumatic event followed by development of a bluish translucency of the lower lip is characteristic of mucus extravasation phenomenon, other lesions might be considered when a typical history is absent. These include salivary gland neoplasm (especially mucoepidermoid carcinoma), vascular malformation, venous varix, and soft tissue neoplasm such as neurofibroma or lipoma. Rarely, a mucocele may appear in the alveolar gingival mucosa. When this is the case, an eruption cyst or gingival cyst should be included in the differential diagnosis.
Treatment and Prognosis
The treatment of mucus extravasation phenomenon is surgical excision. Aspiration of the fluid content provides no lasting clinical benefit. Removal of the associated minor salivary glands along with the pooled mucus is necessary to prevent recurrence. No treatment is required for superficial mucoceles, since they rupture spontaneously and are short-lived.












{kind=link}